HIPEC for Ovarian Cancer – Advanced Treatment for Complex Disease
HIPEC (Hyperthermic Intraperitoneal Chemotherapy) represents one of the most significant advances in treating advanced ovarian cancer. This specialized technique combines complete surgical removal of visible cancer with delivery of heated chemotherapy directly into the abdomen, targeting microscopic disease that remains after surgery.
Dr. Aiswarya Sekar has extensive HIPEC experience, having performed over 100 procedures during her training at Tata Memorial Hospital. She brings this advanced expertise to carefully selected patients who may benefit from this intensive but potentially life-extending treatment.
Understanding HIPEC
HIPEC is not a standalone treatment but rather an addition to cytoreductive surgery for advanced ovarian cancer. The procedure involves:
- Cytoreductive Surgery – Removal of all visible cancer from abdomen and pelvis through complex surgical techniques
- Heated Chemotherapy Bath – Once cancer removal is complete, heated chemotherapy solution (typically 41-43°C) is circulated throughout the abdominal cavity for 60-90 minutes
- Direct Cancer Cell Kill – Heat and chemotherapy work synergistically to destroy microscopic cancer cells that may remain after surgery
How HIPEC Works
The Heat Effect
Heating chemotherapy to 41-43 degrees Celsius provides several advantages:
- Cancer cells are more sensitive to heat than normal cells
- Heat increases chemotherapy penetration into tissues
- Heat enhances chemotherapy cytotoxic effects
- Synergistic cancer cell destruction
Direct Delivery Advantage
Traditional intravenous chemotherapy must travel through bloodstream to reach cancer cells, limiting concentration at tumor sites. HIPEC delivers chemotherapy:
- Directly to abdominal surfaces where microscopic disease remains
- At concentrations 20-1000 times higher than achievable through IV chemotherapy
- With minimal systemic absorption, reducing side effects
Targeting Microscopic Disease
Even after complete removal of all visible cancer during cytoreductive surgery, microscopic cancer cells often remain on peritoneal surfaces. These cells, invisible to the naked eye, cause cancer recurrence. HIPEC specifically targets this microscopic residual disease.
Who Benefits from HIPEC?
HIPEC is not appropriate for all ovarian cancer patients. Careful patient selection is essential. Potential candidates include:
Primary Setting
- Advanced ovarian cancer (Stage III-IV)
- After neoadjuvant chemotherapy with good response
- When complete or near-complete cytoreduction is achievable
- Good overall health and performance status
Recurrent Setting
- Platinum-sensitive recurrent disease
- Disease-free interval of at least 6 months since prior chemotherapy
- Limited number of recurrence sites
- Complete resection appears feasible
Hipec For Ovarian Cancer
HIPEC is not recommended for patients with:
- Extensive liver metastases
- Extra-abdominal disease
- Poor response to chemotherapy
- Significant medical comorbidities
- Performance status too poor to tolerate major surgery
Dr. Aiswarya carefully evaluates each patient’s imaging studies, chemotherapy response, overall health, and disease characteristics to determine HIPEC candidacy.
The HIPEC Procedure
Preoperative Preparation
Before HIPEC, patients undergo:
- Comprehensive medical evaluation
- Optimization of nutrition and overall health
- Imaging studies to plan surgery
- Detailed discussion of procedure, risks, and expected outcomes
- Coordination with anesthesiology and intensive care teams
The Surgery
HIPEC procedures typically take 6-10 hours and involve:
Exploration – Systematic examination of entire abdomen to assess disease extent
Cytoreductive Surgery – Removal of all visible cancer, which may include:
- Removal of ovaries, uterus, fallopian tubes
- Omentectomy (removal of fatty abdominal tissue)
- Peritonectomy (removal of peritoneal lining from diaphragm, pelvis, abdominal walls)
- Bowel resection if tumor involves intestines
- Diaphragm stripping
- Liver capsule resection
- Spleen removal in some cases
- Lymph node removal
Assessment of Cytoreduction – Determining whether complete or optimal cytoreduction achieved. HIPEC should only proceed if minimal residual disease remains.
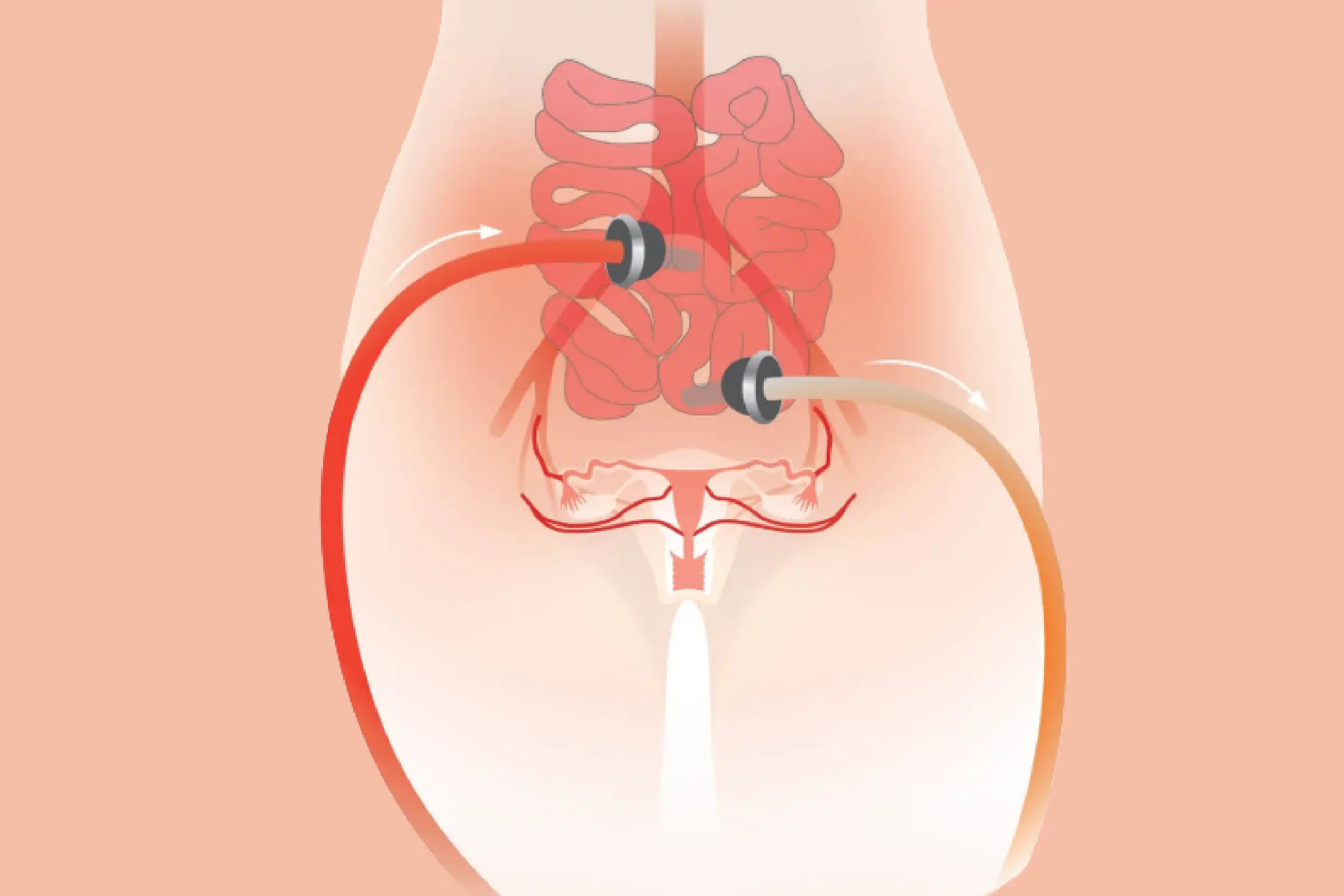
HIPEC Delivery – Once cytoreduction complete:
- Catheters placed in abdomen
- Abdominal incision temporarily closed
- Heated chemotherapy circulated for 60-90 minutes
- Continuous monitoring of temperature and patient vital signs
Final Steps – After HIPEC:
- Removal of chemotherapy solution
- Thorough washing of abdomen
- Bowel reconstruction if needed
- Permanent closure of incision
Recovery
HIPEC requires intensive initial recovery:
- ICU monitoring for 24-48 hours
- Hospital stay typically 7-14 days
- Management of fluid shifts and electrolyte imbalances
- Nutritional support
- Pain management
- Gradual return of bowel function
- Physical therapy and mobilization
Most patients return to baseline activity by 6-8 weeks after surgery.
Chemotherapy Agents Used
Common chemotherapy agents for ovarian cancer HIPEC include:
- Cisplatin – Most commonly used, excellent penetration
- Carboplatin – Alternative platinum agent
- Paclitaxel – Sometimes combined with platinum
Agent selection depends on individual factors, prior chemotherapy received, and institutional protocols.
Risks and Complications
HIPEC is a major procedure with significant risks:
Surgical Risks
- Bleeding requiring transfusion
- Bowel injury or anastomotic leak
- Pancreatic or splenic injury
- Wound complications
- Blood clots
HIPEC-Specific Risks
- Bone marrow suppression
- Kidney dysfunction
- Electrolyte imbalances
- Hypothermia or hyperthermia
General Risks
- Infection
- Need for reoperation
- Prolonged ileus (bowel dysfunction)
- ICU admission
- Mortality risk (1-3% in experienced centers)
Dr. Aiswarya thoroughly discusses these risks, ensuring patients understand the intensive nature of HIPEC before proceeding.
Expected Outcomes
Survival Benefits

Studies of HIPEC in ovarian cancer show:
- Improved progression-free survival compared to surgery alone
- Potential overall survival advantage in selected patients
- Best outcomes when complete cytoreduction achieved
- Benefits most pronounced in platinum-sensitive recurrent disease
Quality of Life
While HIPEC involves longer recovery than surgery alone:
- Most patients return to good quality of life within 2-3 months
- Potential for longer disease-free intervals
- Reduced need for repeated chemotherapy in some cases
After HIPEC: What Comes Next
Adjuvant Chemotherapy
Following HIPEC, most patients receive additional systemic chemotherapy:
- Usually begins 4-6 weeks after surgery
- Completes the planned chemotherapy course
- Addresses potential microscopic disease outside abdomen
Surveillance
After completing all treatment:
- Regular follow-up examinations
- CA-125 monitoring
- Imaging studies as indicated
- Prompt evaluation of new symptoms
Recurrence Management
If cancer recurs after HIPEC:
- Further surgery generally not recommended
- Systemic chemotherapy remains primary treatment
- Clinical trial consideration
- Focus on quality of life and symptom management
HIPEC vs. Standard Treatment
Patients often ask whether HIPEC is better than standard surgery and chemotherapy. The answer depends on individual circumstances:
Advantages of HIPEC
- May improve progression-free survival
- Delivers higher chemotherapy concentrations to abdominal surfaces
- May extend time before recurrence
Considerations
- More intensive surgery and recovery
- Higher complication risk
- Not appropriate for all patients
- Requires experienced surgical team
Dr. Aiswarya helps patients understand whether HIPEC’s potential benefits outweigh risks in their specific situation.
Why Experience Matters
HIPEC is technically demanding, requiring:
- Expertise in complex cytoreductive surgery
- Experience with upper abdominal procedures
- Understanding of HIPEC protocols and chemotherapy delivery
- Ability to manage potential complications
- Multidisciplinary team support
Centers performing high volumes of HIPEC procedures demonstrate better outcomes and lower complication rates. Dr. Aiswarya’s training at India’s largest cancer center provided extensive HIPEC experience with over 100 procedures, preparing her to offer this treatment safely and effectively.
The Decision Process
Deciding whether to proceed with HIPEC requires careful consideration:
Questions to Discuss
- Am I a good candidate based on disease characteristics?
- What are realistic expectations for outcomes?
- What does recovery involve?
- What are my alternatives?
- How does HIPEC fit into my overall treatment plan?
Shared Decision-Making
Dr. Aiswarya believes in comprehensive counseling, ensuring patients understand:
- The intensive nature of HIPEC
- Realistic outcome expectations
- Alternative treatment options
- Individual risk-benefit balance
Only after thorough discussion and mutual agreement does HIPEC proceed.
Second Opinions for HIPEC
Given HIPEC’s complexity and intensity, seeking expert evaluation is reasonable if:
- You’ve been told HIPEC is your only option
- You’re uncertain whether you’re a good candidate
- You want confirmation of surgical plan
- You need help deciding between options
Dr. Aiswarya welcomes second opinion consultations, providing objective assessment and recommendations based on current evidence.
Hope Through Innovation
While ovarian cancer remains challenging, advances like HIPEC offer hope for improved outcomes in advanced disease. For carefully selected patients, this intensive treatment provides opportunity for longer disease-free survival and extended life.
Dr. Aiswarya’s extensive HIPEC experience, combined with comprehensive ovarian cancer expertise, ensures patients receive evidence-based recommendations and expert surgical care when HIPEC is appropriate.
If you have advanced ovarian cancer and want to understand whether HIPEC might be appropriate for your situation, specialized consultation can provide clarity. Contact us today to schedule an appointment.